Bundibugyo: The Ebola Strain the World Was Not Prepared For
The Bundibugyo virus is the most recently discovered species of orthoebolavirus. It was first identified in 2007. It has occurred in only three documented outbreaks in its entire recorded history. It has no approved vaccine. It has no approved therapeutic. Its case fatality rate ranges from 25 to 50 per cent. As of 19 May 2026, it has killed at least 116 people and infected nearly 500 suspected cases across Ituri Province in the DRC and reached Uganda's capital Kampala. The WHO has declared a public health emergency of international concern. The standard Ebola response toolkit built over five decades cannot be directly applied. The Meridian Intelligence Desk explains what Bundibugyo is, where it comes from, how it spreads, what it does to the human body and what the absence of any approved countermeasure actually means in a conflict zone.
When the world hears the word Ebola, it thinks of the Zaire strain. The catastrophic 2014 to 2016 West Africa epidemic that killed over 11,000 people. The 2018 to 2020 DRC outbreak that killed approximately 2,300. The images of isolation units, protective suits and the terrifying haemorrhagic fever that has defined public understanding of the disease since the virus was first identified in 1976 near the Ebola River in what is now the DRC. That mental model is built around Zaire. It shapes the pharmaceutical investments that produced Ervebo, the first approved Ebola vaccine. It shapes the clinical trial programmes that produced the REGN-EB3 and mAb114 antibody therapeutics. It shapes the stockpiles that national governments and the WHO maintain for emergency deployment. The problem is that Bundibugyo is not Zaire. It is a distinct viral species with its own characteristics, its own transmission dynamics, its own history and, most critically, its own complete absence from the pharmacological response architecture that the world built for Ebola. When Bundibugyo arrived in Ituri Province in May 2026, it found the international health system holding a toolbox built for a different disease.
Up from 246 on 16 May. Rapidly evolving. NBC News 19 May
Up from 88 on 17 May. CDC and UN data 19 May 2026
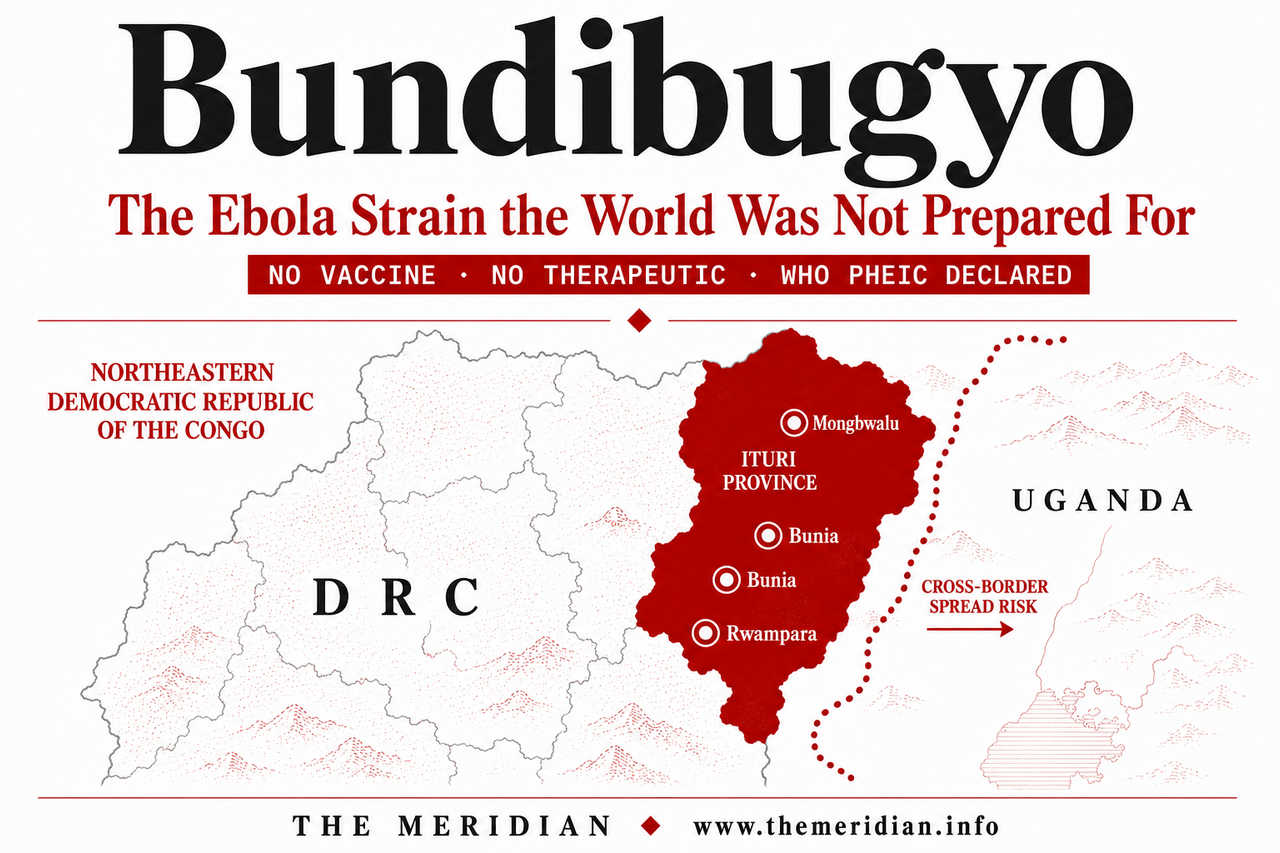
Including Bunia, Rwampara, Mongbwalu. CDC 18 May
Past two outbreaks 2007 and 2012. WHO and CDC
2007 Uganda. 2012 DRC. 2026 DRC. WHO outbreak history
Ervebo and REGN-EB3 only work against Zaire strain
Bundibugyo virus definition orthoebolavirus species discovery history reservoir fruit bat
The Bundibugyo virus, formally designated Orthoebolavirus bundibugyoense, is one of four species of orthoebolavirus known to cause disease in humans. The other three are the Zaire virus, the Sudan virus and the Tai Forest virus, the last of which has caused only a single documented human infection in recorded history. Bundibugyo is the most recently discovered of the four. It was identified in November 2007 when scientists at the United States Centers for Disease Control and Prevention and the Uganda Virus Research Institute characterised samples from an outbreak in Bundibugyo district in western Uganda. It was immediately recognised as a new species, genetically distinct from all previously known ebolaviruses. Phylogenetic analysis showed it was most closely related to the Tai Forest virus but represented a separate evolutionary lineage within the Orthoebolavirus genus.
Like all ebolaviruses, Bundibugyo is a member of the Filoviridae family — the same family that includes Marburg virus. Filoviruses are characterised by their distinctive filamentous structure, visible under electron microscopy as long, thread-like particles that can appear as hooks, loops or the characteristic shepherd's crook shape. They carry a single-stranded, negative-sense RNA genome. The presumed natural reservoir for Bundibugyo, as for the other ebolaviruses, is fruit bats of the Pteropodidae family. The reservoir has not been definitively confirmed for Bundibugyo specifically, but the evidence for fruit bats as the primary wildlife reservoir for ebolaviruses is strong across the genus, based on serological studies and virus isolation from bat populations in affected regions. The virus enters human populations through direct contact with infected animals, most commonly through the handling of sick or dead wildlife including non-human primates, porcupines and fruit bats found in or near the rainforest. From that initial spillover event, human-to-human transmission then sustains the outbreak.
Bundibugyo outbreak history 2007 Uganda 2012 DRC 2026 DRC Ituri timeline
Bundibugyo symptoms fever haemorrhagic fever vomiting bleeding incubation period clinical presentation
Bundibugyo virus disease is a severe haemorrhagic fever. The clinical presentation follows a recognisable progression that begins with symptoms easily confused with many other febrile illnesses and escalates, in severe cases, to systemic haemorrhage and multi-organ failure. The incubation period, the time from exposure to the onset of symptoms, ranges from two to 21 days. Most cases present between four and ten days after exposure.
The early phase typically presents suddenly with high fever, severe headache, fatigue, muscle pain, sore throat and weakness. These symptoms are non-specific and closely resemble influenza, malaria and many other tropical febrile illnesses common in the DRC. This non-specificity is one of the most dangerous features of Bundibugyo in the specific context of Ituri Province, where malaria, typhoid and other febrile diseases are endemic and where patients and healthcare workers may not initially recognise Bundibugyo symptoms as distinct from more common illnesses. In settings with limited laboratory capacity, this diagnostic uncertainty delays isolation and increases transmission risk.
The middle phase, typically beginning four to five days after symptom onset, introduces the more characteristic haemorrhagic features. Patients develop vomiting, diarrhoea, rash and severe abdominal pain. The diarrhoea can be profuse and rapidly leads to dehydration and electrolyte imbalance. The rash, typically a maculopapular eruption appearing first on the face and trunk, is a useful diagnostic indicator when present. As the disease progresses, nosebleeds, vomiting of blood and bleeding from other sites including the gums, injection sites and mucous membranes may occur. In the current DRC outbreak, patients have experienced classic Ebola disease symptoms including fever, headache, vomiting, severe weakness, abdominal pain, nosebleeds and vomiting of blood, according to the CDC. The final phase in fatal cases involves multi-organ failure, shock and death, typically between six and sixteen days after symptom onset. Survivors begin to recover after this period, though recovery is slow and prolonged fatigue, muscle weakness and psychological effects are common. Viral RNA can persist in certain body fluids including semen for extended periods after clinical recovery, creating transmission risk during convalescence.
Bundibugyo begins like malaria and ends like nothing else. In a region where malaria is ubiquitous, the diagnostic window in which isolation can interrupt transmission is narrow, brief and difficult to recognise.
Bundibugyo transmission bodily fluids healthcare workers burial practices bushmeat DRC
Bundibugyo spreads through direct contact with the blood, bodily fluids or secretions of an infected person. The virus is present in blood, saliva, urine, sweat, faeces, vomit, breast milk and semen of infected individuals. Transmission requires direct mucous membrane or broken skin contact with these fluids, or indirect contact through contaminated surfaces, materials or objects including bedding, clothing, medical equipment and needles. Unlike respiratory viruses, Bundibugyo does not spread through casual contact or through the air under normal circumstances. Droplet transmission in close proximity to a severely ill patient generating aerosols through vomiting or coughing may occur but is not the primary transmission route and requires close proximity rather than distant airborne spread.
Healthcare workers are at substantially elevated risk. The nurse who is believed to be the index case of the current outbreak died at the Evangelical Medical Centre in Bunia. Healthcare worker infection is a recognised feature of all previous Bundibugyo outbreaks and of Ebola outbreaks generally, reflecting the high viral loads in severely ill patients, the intimate care requirements of haemorrhagic fever patients and the frequent inadequacy of personal protective equipment in resource-limited settings. In the 2007 Uganda outbreak, healthcare worker infections were documented among staff who had contact with patients without adequate protection. Safe burial practices are a critical intervention because viral load in the bodies of deceased patients remains high and traditional burial practices involving direct contact with the body create significant transmission risk. Community resistance to safe burial protocols, rooted in cultural and religious practices, has been a documented challenge in previous DRC Ebola responses.
Bundibugyo no vaccine pharmaceutical development neglected disease economics Zaire Ervebo clinical trial
The absence of a Bundibugyo vaccine is not a scientific failure. It is an economic one. Vaccine development requires sustained investment over years, driven by assessments of commercial market size, outbreak frequency, geopolitical priority and the probability of regulatory approval. The calculus for Bundibugyo, before May 2026, produced an answer of insufficient investment on every dimension. The Bundibugyo strain had caused two outbreaks in its entire recorded history before the current crisis, with a combined total of 226 cases across both events. That case count, spread across nearly two decades, did not generate the market signal, the political urgency or the public health investment that produces vaccine development programmes.
The Zaire strain is the reason Ervebo exists. The 2014 to 2016 West Africa epidemic, with over 28,600 cases and 11,000 deaths across Guinea, Sierra Leone and Liberia, produced the combination of political pressure, emergency funding and accelerated regulatory pathways that drove the Ervebo vaccine from Phase I trials to regulatory approval in five years. The 2018 to 2020 DRC outbreak, the second largest in history, provided the field deployment data that confirmed Ervebo's efficacy and supported its full licensure by both the European Medicines Agency and the US Food and Drug Administration in 2019. The REGN-EB3 and mAb114 antibody therapeutics were developed through the same emergency pipeline, driven by the same scale event. Bundibugyo never had its 2014 moment. It never generated the political and financial mobilisation that produces countermeasures. It remained, in the pharmaceutical development landscape, a neglected pathogen.
Emergency clinical trials for Bundibugyo-specific countermeasures are now being initiated in response to the 2026 outbreak. Several research groups have candidate therapeutic approaches based on platform technologies that have been applied to Zaire, and some preliminary work on Bundibugyo-specific monoclonal antibodies exists in research settings. But translating a research candidate into an approved therapeutic requires years under normal conditions and months even under emergency use authorisation frameworks. The outbreak is happening now. The clinical trials are beginning now. The people in Ituri Province are sick now. The gap between the disease calendar and the pharmaceutical development calendar is the most consequential structural feature of the current emergency.
Bundibugyo DRC response no vaccine conflict zone Ituri M23 healthcare capacity WHO MSF
For the Zaire strain, the response toolkit includes ring vaccination — deploying Ervebo to all confirmed contacts of a confirmed case and all contacts of those contacts, creating a protective ring around the outbreak that slows and ultimately halts transmission. During the 2018 to 2020 DRC outbreak, ring vaccination was deployed despite active conflict and was a primary tool in eventually controlling an outbreak that at its peak was producing hundreds of new cases per week. For the current Bundibugyo outbreak, ring vaccination is not possible. There is no ring to vaccinate with. Every contact of every confirmed case in Ituri Province is unprotected. Every healthcare worker treating Bundibugyo patients is relying entirely on personal protective equipment, the adequacy of which in the specific facilities of conflict-affected Ituri Province cannot be assumed.
The response in the absence of pharmaceutical countermeasures falls back on the classic public health triad that has been the foundation of Ebola control since 1976: case detection, isolation and contact tracing. Find every case as quickly as possible. Isolate every confirmed and suspected case in a dedicated treatment facility. Trace every person who had contact with every case and monitor them for 21 days. Safe burial of all deceased cases. Community engagement to overcome resistance and ensure that suspected cases present to health facilities rather than seeking care from informal providers or traditional healers where infection prevention and control measures cannot be applied. These measures work. They controlled all sixteen previous DRC Ebola outbreaks, including the massive 2018 to 2020 crisis. They require access, logistics, community trust, trained staff and functioning laboratory capacity to work. In conflict-affected Ituri Province, with M23 active in adjacent areas, with the large network of informal healthcare facilities documented by the WHO as a significant amplification risk, and with population displacement creating contact tracing chains that extend across provincial and international borders, each of these requirements is under stress simultaneously.
The suspected index case was a nurse. The nurse accessed a formal healthcare facility. The healthcare facility identified the cluster. The laboratory in Kinshasa confirmed Bundibugyo. The response machinery activated. By the time it activated, the WHO's own analysis indicated that eight of the initial 13 samples collected tested positive, suggesting a positivity rate that points toward a potentially much larger outbreak than what was initially detected. The gap between the biological reality and the institutional response is the space in which the outbreak grew from its first cases to nearly 500 suspected cases in two weeks. That gap is not a failure of any individual institution. It is the structural consequence of a neglected pathogen meeting a constrained response environment with no pharmacological tools to compress the detection-to-isolation interval that ultimately determines outbreak size.
Bundibugyo was a virus the world had 19 years to prepare for. It had two outbreaks between 2007 and 2026 and killed 73 people combined. No vaccine was developed. No therapeutic was approved. In May 2026, it is killing people at ten times that rate. The window that was not used is now closed.
Add comment
Comments