Two Viruses, One Month: Ebola Bundibugyo in the DRC and Hantavirus on the High Seas
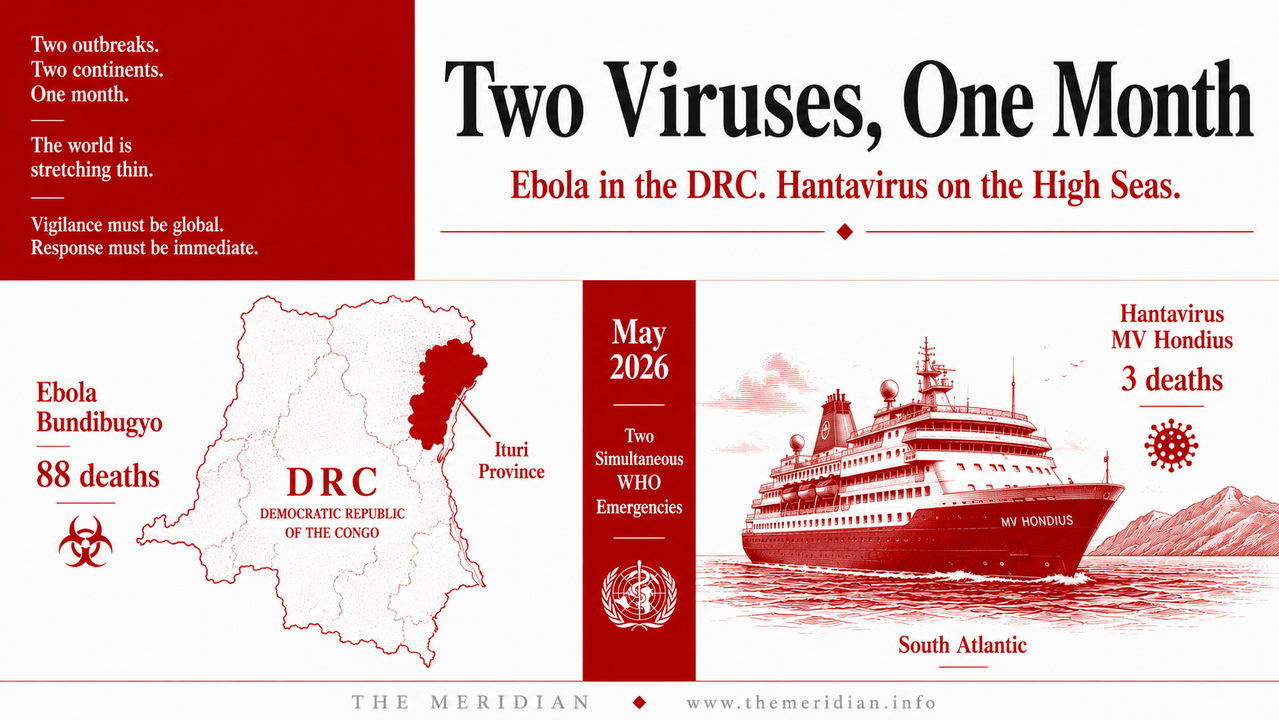
On 17 May 2026, the WHO declared a public health emergency of international concern over the Ebola Bundibugyo outbreak in the DRC. By 18 May, 88 people were dead and 336 cases suspected across Ituri Province and beyond. No approved vaccine exists for this strain. Simultaneously, the MV Hondius cruise ship hantavirus cluster has killed three and infected passengers from 23 nationalities across 15 countries — the first hantavirus outbreak on a cruise ship in recorded history. The Meridian Intelligence Desk analyses both outbreaks, what they reveal about global health security and what the DRC's capacity to respond actually looks like.
The world in May 2026 is simultaneously managing an Iran war oil shock, the most geographically widespread economic disruption since 1870, a water crisis on a small island in the Indian Ocean and now two concurrent viral emergencies declared by the World Health Organization in the same month. The simultaneity is not accidental. It reflects a structural reality about the current global moment: the multilateral institutions designed to manage individual crises are being tested by the compounding of crises in a way that their architectures were never designed to absorb. Ebola Bundibugyo in the DRC is the most serious of the two viral emergencies by scale and systemic risk. Hantavirus Andes on the MV Hondius is the more scientifically unusual. Together they illustrate with precision how a world distracted by geopolitical fires can be simultaneously confronted by the biological emergencies that have always been the most democratic of threats: they do not respect borders, alliances, debt ratings or strategic access agreements.
336 suspected cases. 11 confirmed. WHO PHEIC declared 17 May
Only 3rd occurrence of Bundibugyo strain globally
Unlike Zaire strain which has Ervebo vaccine and REGN-EB3
3 deaths. 8 confirmed cases. First cruise ship outbreak in history
Ebola Bundibugyo DRC 2026 Ituri Province no vaccine strain difference Zaire symptoms transmission
Ebola is not a single disease caused by a single virus. It is a group of severe illnesses caused by several distinct viral species within the Orthoebolavirus genus, each with its own geographic origin, transmission characteristics, case fatality rate and, critically, its own susceptibility to the countermeasures that the global health system has developed over five decades of response experience. The distinction matters enormously in the context of the current DRC outbreak because the standard Ebola response toolkit was built around the Zaire strain, which has caused the majority of the 17 Ebola outbreaks in the DRC since 1976, including the catastrophic 2014 to 2016 West Africa epidemic that killed over 11,000 people and the 2018 to 2020 DRC outbreak that killed approximately 2,300.
For the Zaire strain, approved medical countermeasures exist. The Ervebo vaccine provides pre-exposure protection and has been deployed in ring vaccination campaigns that significantly reduced transmission during the 2018 to 2020 outbreak. The REGN-EB3 and mAb114 antibody cocktails have been approved as treatments that significantly improve survival rates for infected patients. Healthcare workers can be vaccinated. Contacts can be vaccinated. The medical response has a pharmacological anchor that changes the arithmetic of containment. The Bundibugyo strain has none of this. It was first identified in Uganda in 2007, occurred a second time in the DRC in 2012 and is now occurring for only the third time in recorded history. The existing Ebola vaccines and antibody therapeutics were developed specifically for the Zaire strain. They offer little or no protection against Bundibugyo. Healthcare workers entering isolation units to treat Bundibugyo patients are relying entirely on personal protective equipment, infection prevention and control protocols and supportive care. Emergency clinical trials for Bundibugyo-specific countermeasures are being initiated, but clinical trials take months. The outbreak is happening now.
The symptoms of Bundibugyo virus disease follow the characteristic Ebola pattern: sudden onset of fever, severe headache, muscle pain, weakness and fatigue, followed by vomiting, diarrhoea, rash and in severe cases bleeding from multiple sites. The incubation period is two to 21 days. The case fatality rate for Bundibugyo in historical outbreaks has ranged from approximately 25 to 36 per cent. The 2026 DRC outbreak's current case fatality rate among suspected cases is consistent with this historical range. Transmission occurs through direct contact with the blood, bodily fluids or secretions of infected people and through contact with surfaces and materials contaminated with these fluids. Unlike influenza or Covid-19, Ebola does not spread through casual contact or through the air in normal circumstances. This is the fundamental reason that Ebola outbreaks, while locally devastating, have not historically produced global pandemics: the transmission requirement of direct contact with bodily fluids is a natural limiting factor that respiratory viruses do not face.
DRC Ebola response capacity Ituri conflict healthcare infrastructure WHO CDC MSF
The DRC has more experience managing Ebola outbreaks than any other country in the world. Seventeen outbreaks since 1976 have produced an institutional knowledge base, a cadre of trained health workers, a network of laboratories and an Ebola response coordination architecture that is genuinely the most developed in the world for this specific disease. The National Institute for Biomedical Research in Kinshasa, led by Professor Jean-Jacques Muyembe who co-discovered the Ebola virus in 1976, has the scientific expertise and the laboratory infrastructure to confirm cases and support response coordination. The DRC government has activated its public health emergency operations centre, strengthened epidemiological and laboratory surveillance, and deployed response teams to Ituri Province.
The constraints are structural and simultaneous. The outbreak is centred in Ituri Province in northeastern DRC, one of the most conflict-affected regions on the continent. The M23 militia controls significant portions of eastern DRC including areas adjacent to the current outbreak zone. Active insecurity limits access for response teams, complicates contact tracing and creates population displacement that accelerates transmission. The affected areas of Ituri Province are logistically challenging regions with limited transportation infrastructure, difficult terrain and ongoing security concerns that complicate access for response teams and medical personnel. A confirmed case in Goma, the commercial hub of North Kivu that is under M23 control, was announced on 17 May, involving the wife of a man who died of Ebola in Bunia and who travelled to Goma after her husband's death whilst already infected. This specific transmission event illustrates precisely how conflict-driven population movement creates transmission chains that contact tracing cannot easily interrupt.
The large network of informal healthcare facilities in Ituri Province, where patients seek care from traditional healers and informal providers before or instead of presenting to formal health facilities, is identified by the WHO as a significant amplification risk. The suspected index case was a nurse who died at the Evangelical Medical Centre in Bunia, suggesting that healthcare worker transmission within formal facilities is already occurring. The high positivity rate of initial samples collected, with eight positives among 13 samples collected in various areas, points toward a potentially much larger outbreak than what is currently being detected and reported. International support through the WHO, the CDC, Médecins Sans Frontières and the Africa CDC is substantial. But the combination of Bundibugyo-specific countermeasure absence, active conflict, informal healthcare networks and high population mobility creates a response environment of exceptional difficulty.
The DRC has fought Ebola seventeen times. It has never fought Bundibugyo while simultaneously managing M23 in the same province, with no approved vaccine, and with a confirmed case already in Goma.
Hantavirus Andes virus MV Hondius cruise ship 2026 human transmission symptoms WHO CDC
The MV Hondius outbreak is scientifically remarkable for a specific and narrow reason: it is the first documented hantavirus outbreak on a cruise ship in recorded history, and it involves the only known hantavirus species capable of human-to-human transmission. Most hantaviruses infect humans through contact with infected rodents, specifically through inhalation of aerosols from infected rodent urine, faeces or saliva. A person cleans out a cabin that has been closed for winter, disturbs dried rodent droppings and inhales virus particles. This is the standard transmission route, and it is why hantavirus infection in humans is typically an isolated individual event rather than an outbreak in the epidemiological sense.
The Andes virus is the exception. Found naturally in Argentina and Chile, it is the only hantavirus species that has been documented to spread from person to person, through close sustained contact, potentially including airborne transmission in poorly ventilated settings. The MV Hondius departed from Ushuaia, Argentina, on 1 April 2026 and visited remote areas including Antarctica, South Georgia Island, Tristan da Cunha, Saint Helena and Ascension Island. The index case, a 70-year-old Dutch man, fell ill on 6 April with fever, headache, abdominal pain and diarrhoea. He developed respiratory distress and died onboard on 11 April. The WHO's working hypothesis is that he acquired the infection prior to boarding through environmental exposure during activities in Argentina, with subsequent human-to-human transmission among passengers onboard. By the time the outbreak was reported to the WHO on 2 May, three people were dead and the virus had reached passengers from 23 nationalities across six continents.
As of 13 May 2026, eight confirmed cases and three suspected cases directly linked to the outbreak had been reported, with three deaths. Former passengers were hospitalised or quarantined in Australia, Canada, France, Germany, the Netherlands, Saint Helena, Singapore, South Africa, Spain, Switzerland, Turkey and the United States. An American who tested positive was moved to Germany for treatment. British military personnel from the 16 Air Assault Brigade parachuted to Tristan da Cunha, one of the most remote inhabited islands on earth, to reach a suspected case among its 220 residents. This is the geography of global connectivity expressed as epidemiological risk: a rodent in a field in Patagonia, a cruise ship passenger who encountered its droppings, 147 passengers from 23 countries, and within six weeks military parachute operations on a remote South Atlantic island.
Ebola hantavirus comparison global health security 2026 WHO response countermeasures
global health security 2026 simultaneous crises WHO PHEIC multilateral institutions response capacity
The most important analytical observation about May 2026's two simultaneous viral emergencies is not about the viruses themselves. It is about the structural conditions that allowed them to emerge and spread simultaneously while the world's attention was directed elsewhere. The Iran war oil shock has consumed the diplomatic bandwidth of every major power. The DRC's ongoing M23 conflict, documented in The Meridian's Africa Intelligence Brief and Africa's Mineral Paradox articles this month, has degraded the healthcare infrastructure in precisely the region where the Ebola Bundibugyo outbreak is now centred. The conflict-driven population displacement that makes contact tracing in Ituri Province so difficult is itself a product of the mineral extraction competition that The Meridian identified as the fundamental driver of eastern DRC's instability.
The hantavirus outbreak illustrates a different structural dimension of global health risk: the connectivity that makes modern economic life possible, specifically the cruise ship industry that allows 147 people from 23 nationalities to travel together across six continents in a single month, is simultaneously the connectivity that moves a zoonotic virus from a Patagonian rodent to a hospital in Singapore within weeks. This is not a criticism of cruise ships. It is a description of the world as it actually exists. Global connectivity is the condition that makes the Iran war's oil shock felt in Mauritius. It is the condition that makes a Patagonian rodent's Andes virus transmissible on a Dutch cruise ship in the South Atlantic. It is the same condition that allowed Covid-19 to reach every country on earth within months of its emergence in Wuhan.
The global health security architecture that exists to manage these risks is the WHO, supported by national public health agencies including the CDC, Africa CDC and ECDC, operating through the International Health Regulations framework. That framework has now declared a PHEIC for the Ebola Bundibugyo outbreak, which triggers a set of international coordination obligations, resource mobilisation mechanisms and travel and trade recommendation processes. It is the same framework that was tested by Covid-19, Mpox and the 2022 poliovirus outbreaks in the past five years. Its performance in the DRC Bundibugyo outbreak will be constrained by the same factors that constrain every health response in conflict-affected areas: access, security and the absence of specific countermeasures for a rare strain that the global pharmaceutical development system had no economic incentive to prioritise before the current outbreak began.
Two viruses. One month. One with no vaccine in a conflict zone. One spreading across 23 nationalities on a cruise ship. The world's multilateral institutions were not built for a month like this one. They are managing it anyway. The question is what they build before the next one arrives.
Add comment
Comments